- Research
- Open access
- Published:
Comparative diagnostic performance of VI-RADS based on biparametric and multiparametric MRI in predicting muscle invasion in bladder cancer
BMC Medical Imaging volume 25, Article number: 60 (2025)
Abstract
Background
Vesical Imaging-Reporting and Data System (VI-RADS) based on multiparametric magnetic resonance imaging (mp-MRI) performed well in diagnosing muscle-invasive bladder cancer (MIBC). However, certain cases may present challenges in determining the final VI-RADS score using only T2-weighted imaging (T2WI) and diffusion-weighted imaging (DWI) sequences, especially in the absence of dynamic contrast-enhanced (DCE) imaging. This study aims to evaluates whether biparametric MRI (bp-MRI) achieve comparable diagnostic performance to mp-MRI for predicting MIBC and seeks to identify the most suitable bp-MRI criterion by establishing four specific conditions based on T2WI and DWI.
Methods
A retrospective analysis was conducted on 447 patients who underwent preoperative mp-MRI. Images were evaluated according to the VI-RADS protocol by three independent readers. In the bp-DWI and bp-DWI Plus criteria, DWI was the primary sequence used for lesion assessment, while T2WI was the primary sequence for bp-T2WI and bp-T2WI Plus criteria. The Plus criteria (bp-DWI Plus and bp-T2WI Plus) assigned a final VI-RADS score of 4 when both T2WI and DWI scores were 3. The gold standard for diagnosis was histopathological evaluation after surgery. Diagnostic performance was evaluated by comparing the area under the curve (AUC), sensitivity, specificity, and inter-reader agreement using Cohen’s kappa analysis.
Results
Among 447 patients, 304 confirmed as NMIBC and 143 as MIBC. The kappa values were 0.876, 0.873, 0.873, 0.642, and 0.642 for mp-MRI, bp-DWI, bp-DWI Plus, bp-T2WI, and bp-T2WI Plus, respectively, when VI-RADS cutoff > 2. Similarly, when cutoff > 3, the kappa values were 0.848, 0.811, 0.873, 0.811, and 0.873. No significant differences were observed between mp-MRI and bp-DWI (AUC: 0.916 vs. 0.912, p = 0.498), but mp-MRI and bp-DWI had higher AUCs compared to bp-DWI Plus, bp-T2WI, and bp-T2WI Plus.
Conclusions
Both mp-MRI and bp-DWI demonstrate excellent performance in predicting MIBC, with bp-DWI being an alternative to mp-MRI.
Trial registration
retrospectively.
Background
Bladder cancer is a common malignant tumor of the urinary tract [1]. Compared to non-muscle-invasive bladder cancer (NMIBC), muscle-invasive bladder cancer (MIBC) exhibits greater aggressiveness and has a poorer prognosis [2]. Currently, the diagnosis of MIBC is dependent on diagnostic transurethral resection of bladder tumor (TURBT), which, however, may underestimate the tumor stage [3]. Reported studies indicate that diagnostic TURBT misdiagnoses 0%-32% of MIBCs as NMIBCs [4]. Though repeat-TURBT has been recommended in the case of high-risk NMIBC when necessary, this will undoubtedly increase the risk of complications and financial burden to patients [5].
In 2018, the European Association of Urology published the Vesical Imaging-Reporting and Data System (VI-RADS) based on multiparametric magnetic resonance imaging (mp-MRI) for predicting MIBC [6]. This system establishes a standardized approach to both mp-MRI imaging and reporting for patients with bladder cancer. A previous meta-analysis of 20 studies involving a total of 2725 patients demonstrated that VI-RADS performed well in predicting MIBC, regardless of whether the cutoff value of VI-RADS was > 2 or > 3 [7]. However, mp-MRI is not without limitations. Compared with biparametric magnetic resonance imaging (bp-MRI), mp-MRI demands a longer time for scanning and involves higher cost [8]. Additionally, bp-MRI can reduce the risks associated with the intravenous administration of gadolinium-based contrast agents, including nephrogenic systemic fibrosis, renal failure, and tissue accumulation of gadolinium [9, 10]. Moreover, bp-MRI may be more accurate than mp-MRI for identifying residual disease after neoadjuvant chemotherapy [11].
Currently, a limited number of studies have investigated the value of bp-MRI in evaluating the muscle invasion of bladder cancer [12,13,14,15,16,17]. However, in accordance with the VI-RADS protocol, accurately determining the VI-RADS score is challenging in some cases when relying only on T2-weighted imaging (T2WI) and diffusion-weighted imaging (DWI)/apparent diffusion coefficient (ADC) images. For example, determining whether the VI-RADS score is 2 or 3 can be indeterminate when only T2WI score 3 and DWI score 2 are available [6]. This challenge primarily arises from the lack of dynamic contrast-enhanced (DCE) images, which is one of the most urgent issues to address when attempting to replace mp-MRI with bp-MRI. To date, none of the existing studies have discussed this specific diagnostic scenario, which is systematically explored in the current study.
If VI-RADS based on bp-MRI can achieve or even surpass the diagnostic performance of mp-MRI, it will have substantial value and significance in clinical practice. Therefore, the purpose of this study is to evaluate whether bp-MRI demonstrates comparable diagnostic performance to mp-MRI in predicting MIBC. Furthermore, we have devised four bp-MRI criteria based on specific conditions when exclusively using T2WI and DWI images. Our goal is to identify the most appropriate criterion for using bp-MRI to predict MIBC.
Methods
In accordance with the Declaration of Helsinki, the Ethics Committee of Jiangsu Province Hospital reviewed the study’s design and determined that ethical approval was not required due to its retrospective nature. Consequently, the committee waived the need for formal ethics approval.
Patient population
Retrospective analysis on a total of 533 consecutive patients who underwent TURBT or radical cystectomy from 2013 to 2022 was performed. All the patients underwent surgery within 6 weeks after receiving mp-MRI examination. The specimens underwent pathologic examination. Histologic grade was assessed following the 2004 World Health Organization of urological pathology classification [18]. T stage was assessed following the 2017 Union for International Cancer Control of TNM classification [19]. The following patients were excluded: (a) 8 patients had an interval between mp-MRI examination and surgery longer than 6 weeks; (b) 12 patients received neoadjuvant therapy; (c) 15 patients displayed poor image quality that could not be accurately analyzed for reasons such as severe artifacts, inadequate bladder filling, and an inability to identify tumors; (d) 13 patients were excluded due to a postoperative pathology diagnosis of non-urothelial carcinoma; (e) 7 patients showed undetermined T stage or grade in postoperative pathology; (f) 31 patients could not show detrusor muscle when they underwent TURBT. The final study group consisted of 447 patients in total. The flowchart for selection of the study population is shown in Fig. 1.
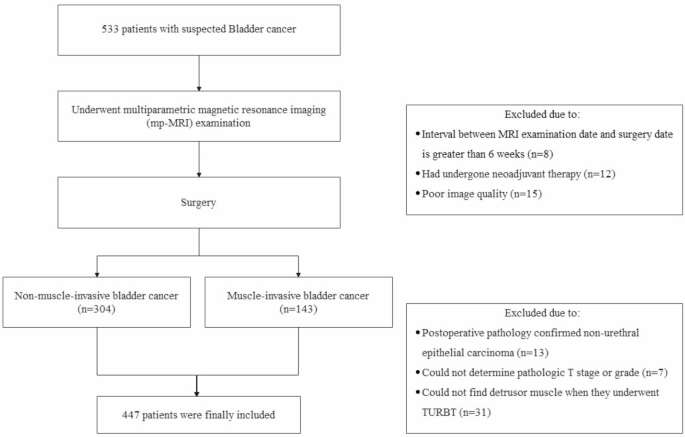
Study flowchart
Multiparameter MRI protocol
MRI scans were performed in a 3.0T MRI system (Ingenia CX; Philips, Netherland) with the use of a 32-channel phased-array surface coil. T2WI were performed with a turbo spin-echo sequence [repetition time/echo time (TR/TE): 4690/119 ms, matrix 320, in-plane spatial resolution: 0.75 × 0.75 mm, slice thickness: 3.0 mm, slice gap: 0.3 mm, and field of view (FOV): 240 mm]. DWI/ADC was conducted with an axial and sagittal/coronal breathing-free spin-echo EPI sequence (TR/TE 4000/61 ms, flip angle 90, matrix 128 × 128, slice thickness: 3.0 mm, and FOV: 240 mm). B value was set between 0 and 2000 s/mm2 (0, 50, 700, 1400, and 2000). DCE was performed with a 3D- THRIVE sequence (TR/TE 3.8/1.2 ms, flip angle 15, matrix 256 × 256, in-plane spatial resolution 0.9 × 0.9 mm, slice thickness 1.0 mm, FOV 240 mm, temporal resolution 8.3 s, and acquisition time 510 s). A single body weight-based dose (0.1 mmol/kg) of gadolinium-based contrast agent (Magnevist, Bayer Healthcare) was intravenously injected at a constant rate of 2.5 mL/second after the fifth dynamic scan, followed by a flush of 25 mL of saline at a flow rate of 2.5 mL/second.
VI-RADS evaluation
All images were analyzed using RadiAnt Dicom Viewer (Version 2021.1, Medixant, Poznan, Poland). The collected images were divided into two sets: one set (Set 1) included axial, sagittal, coronal T2WI along with axial DWI images, the other set (Set 2) included all these images plus axial DCE images. Both sets of the images were evaluated independently by three readers (Reader 1, with more than 2 years of experience; Reader 2, with more than 5 years of experience; Reader 3, with more than 10 years of experience) in two reading sessions. Set 1 was evaluated in the first reading session, and set 2 was in the second. Two reading sessions were separated by at least 4 weeks to avoid recall bias. Readers evaluated lesions according to the VI-RADS protocol for score of T2WI, DWI, and DCE and also for the final VI-RADS score. Final VI-RADS score was determined by Reader 4 (with more than 30 years of experience) if the reading of VI-RADS score differed between the three readers. The readers were blinded to the final pathology results. In cases where patients presented with multiple tumors, the tumor with the highest VI-RADS score was selected for consideration.
Set 1 and set 2 were evaluated according to the VI-RADS protocol. A summary table of the VI-RADS scoring approach is provided in Supplementary Material [6]. According to the VI-RADS protocol, there are two scenarios where determining the final VI-RADS score can be challenging when evaluating set 1 images:
-
T2WI score of 3 and DWI score of 2 (T2WI 3 + DWI 2).
-
Both T2WI and DWI scores of 3 (T2WI 3 + DWI 3).
To address these situations, we established four bp-MRI criteria: bp-DWI, bp-DWI Plus, bp-T2WI, and bp-T2WI Plus.
bp-DWI and bp-DWI Plus prioritize DWI as the dominant sequence for scoring, meaning DWI is the primary determinant when there is a discrepancy (T2WI 3 + DWI 2). bp-T2WI and bp-T2WI Plus prioritize T2WI as the dominant sequence for scoring. In addition, to address the case where both T2WI and DWI scores are 3 (T2WI 3 + DWI 3), we introduced the Plus criteria. The Plus criteria (bp-DWI Plus and bp-T2WI Plus) assign a final VI-RADS score of 4 in this situation.
The detailed differences among the four bp-MRI criteria are shown in Fig. 2. Examples of reader evaluations are shown in Figs. 3 and 4.
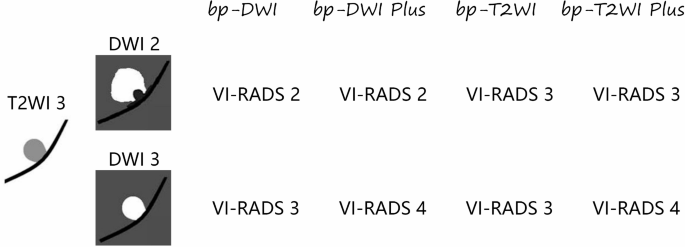
Differences among the bp-MRI criteria of VI-RADS. bp-MRI: biparametric magnetic resonance imaging; VI-RADS: Vesical Imaging-Reporting and Data System
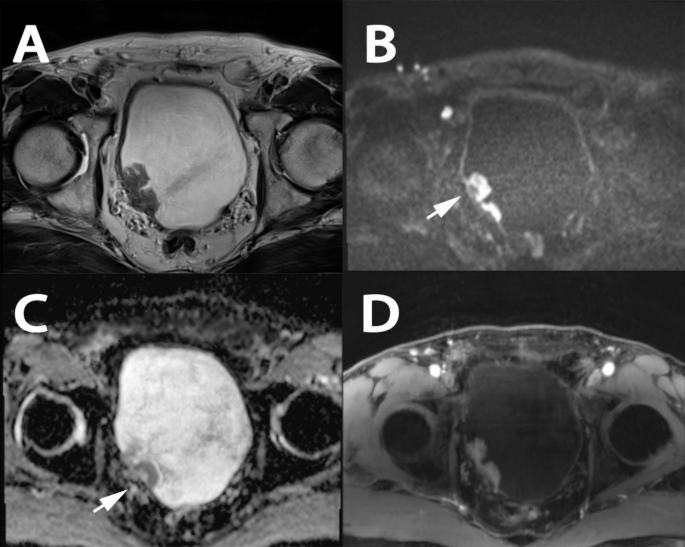
A case demonstrating the use of bp-MRI for determining various scores. A patient over 85 years old with hematuria underwent mp-MRI prior to the initial TURBT. T2WI revealed two sessile tumors without a high signal intensity thickened inner layer on the right bladder wall, with no clear disruption of the low signal intensity muscularis propria observed. Tumors with clear stalks were observed on DWI and ADC (Arrow). Based on bp-MRI, all readers assigned a T2WI category of 3 and a DWI category of 2. However, no clear tumor with stalk was visible on DCE. The final VI-RADS score was determined to be 3. The T stage after TURBT was T1-high grade. A: T2WI; B: DWI; C: ADC; D: DCE. bp-MRI: biparametric magnetic resonance imaging; mp-MRI: multiparametric magnetic resonance imaging; TURBT: transurethral resection of bladder tumor; T2WI: T2-weighted images; DWI: diffusion-weighted imaging; ADC: apparent diffusion coefficient; DCE: dynamic contrast-enhanced; VI-RADS: Vesical Imaging-Reporting and Data System
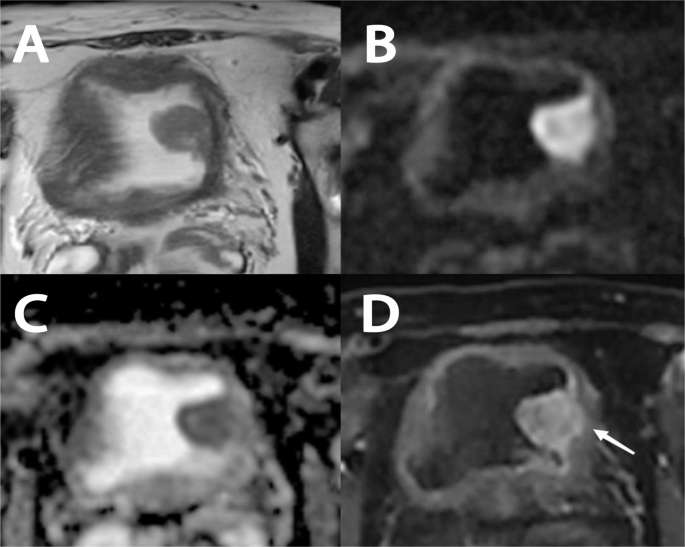
A case demonstrating the use of bp-MRI for determining various scores. A patient over 65 years old with hematuria underwent mp-MRI prior to the initial TURBT. T2WI revealed a sessile lesion on the left bladder wall, measuring more than 2 cm in diameter. No clear disruption of the low signal intensity muscularis propria was observed on T2WI, DWI, or ADC. Based on bp-MRI, all the readers assigned a T2WI category of 3 and DWI category of 3. However, early tumor enhancement extending focally to the muscularis propria was observed on DCE (Arrow). The final VI-RADS score was determined to be 4. The T stage after TURBT was T2-high grade. A: T2WI; B: DWI; C: ADC; D: DCE. bp-MRI: biparametric magnetic resonance imaging; mp-MRI: multiparametric magnetic resonance imaging; TURBT: transurethral resection of bladder tumor; T2WI: T2-weighted images; DWI: diffusion-weighted imaging; ADC: apparent diffusion coefficient; DCE: dynamic contrast-enhanced; VI-RADS: Vesical Imaging-Reporting and Data System
Statistical analysis
Statistical analyses were performed in IBM SPSS software, version 26 (IBM Corporation, Armonk, New York, USA). VI-RADS score > 2 and > 3 served as the cutoff values for diagnose MIBC, respectively. For the assessment of VI-RADS score, inter-reader agreement among the three readers was evaluated using Cohen’s kappa analysis at different cutoff values. Area under the curve (AUC), sensitivity, specificity, positive predictive value, and negative predictive value were used to evaluate each criterion. The AUCs of receiver operating characteristic (ROC) curve comparison was performed using the DeLong test in MedCalc software, version 20 (MedCalc Software Ltd, Acacialaan, Ostend, Belgium). p < 0.05 was considered significant.
Results
The final study group consisted of 447 patients. Detailed information is shown in Table 1. Of the 447 patients, 382 (85.5%) were male, and 65 (14.5%) were female. The median age was 67 years (interquartile range: 26–94 years). A total of 147 patients (32.9%) had multiple bladder lesions (2 or more), accounting for a total of 321 lesions. Of these, 304 patients (68.0%) underwent TURBT and 143 (32.0%) underwent radical cystectomy. 304 patients (68.0%) were pathologically confirmed as NMIBC (Ta-T1) and 143 (32.0%) had MIBC (T2-T4). Specifically, 171 patients (38.3%) were Ta, 133 (29.8%) were T1, 73 (16.3%) were T2, 47 (10.5%) were T3 and 23 (5.1%) were T4. 142 patients (31.8%) were low grade tumor, and 305 patients (68.2%) were high grade tumor.
Five criteria include mp-MRI, bp-DWI, bp-DWI Plus, bp-T2WI and bp-T2WI Plus. The number of patients with VI-RADS 1 and 5 evaluated by the five criteria was 88 patients (19.7%) and 50 patients (11.2%), respectively. VI-RADS 2–4 evaluated by mp-MRI were 173 (38.7%), 63 (14.1%) and 73 (16.3%), respectively. Table 2 shows detailed scores for the five criteria.
The kappa values for inter-reader agreement among the three readers were 0.876, 0.873, 0.873, 0.642, and 0.642 for mp-MRI, bp-DWI, bp-DWI Plus, bp-T2WI, and bp-T2WI Plus, respectively, when using a VI-RADS cutoff score of > 2 (scores 1–2 vs. 3–5). Similarly, the kappa values were 0.848, 0.811, 0.873, 0.811, and 0.873, respectively, when the cutoff was set at > 3 (scores 1–3 vs. 4–5).
Table 3 shows the diagnostic performance of the five criteria across different cutoff values. There were no significant differences observed between mp-MRI and bp-DWI (mp-MRI vs. bp-DWI, AUC: 0.916 vs. 0.912, p = 0.498). However, the AUCs for both mp-MRI and bp-DWI were significantly higher than those for bp-DWI Plus (mp-MRI vs. bp-DWI Plus, AUC: 0.916 vs. 0.900, p = 0.015; bp-DWI vs. bp-DWI Plus, AUC: 0.912 vs. 0.900, p < 0.001), bp-T2WI (mp-MRI vs. bp-T2WI, AUC: 0.916 vs. 0.894, p < 0.001; bp-DWI vs. bp-T2WI, AUC: 0.912 vs. 0.894, p = 0.006), and bp-T2WI Plus (mp-MRI vs. bp-T2WI Plus, AUC: 0.916 vs. 0.896, p = 0.004; bp-DWI vs. bp-T2WI Plus, AUC: 0.912 vs. 0.896, p < 0.001). The ROC curves illustrating the diagnostic performance of the five criteria for predicting MIBC are shown in Fig. 5.

ROC curve in the diagnosis of muscle-invasive bladder cancer for mp-MRI and bp-MRI criteria using VI-RADS. ROC: Receiver Operating Characteristic; mp-MRI: multiparametric magnetic resonance imaging; bp-MRI: biparametric magnetic resonance imaging; VI-RADS: Vesical Imaging-Reporting and Data System
Discussion
Before considering the replacement of mp-MRI with bp-MRI, several critical issues must be addressed. The lack of DCE in bp-MRI raises concerns when using the VI-RADS protocol. For instance, VI-RADS scores can vary if T2WI scores a 3 and DWI scores a 2, or if both T2WI and DWI score a 3 [6]. To identify the optimal criterion for diagnosing MIBC with bp-MRI, we established four criteria based on these variations.
In 2021, Delli et al. [12] were the first to to compare bp-MRI and mp-MRI for diagnosing MIBC, finding no significant difference in diagnostic performance between the two, regardless of the reader’s experience. Similarly, A meta-analysis of 17 studies with 2344 patients showed comparable diagnostic efficacy between bp-MRI and conventional VI-RADS for MIBC [20]. Our findings also indicate no significant difference between mp-MRI and bp-DWI in diagnosing MIBC.
The primary difference between bp-DWI and bp-T2WI is their reliance on different imaging sequences: bp-DWI depends on DWI, while bp-T2WI relies on T2WI. Our results show that bp-DWI outperforms bp-T2WI in diagnostic accuracy. This may be due to the clearer distinction between lesion and muscle layer on DWI compared to T2WI, where inflammatory edema can obscure the evaluation. Tekes et al. [21] reported that 81% of tumors showed a signal intensity similar to that of the muscle layer on T2WI. When the bladder wall has inflammatory edema on T2WI, evaluating the relationship between lesion and muscle layer becomes more difficult [22]. In contrast, the lesion shows a high signal intensity and the muscle layer shows a low and medium signal intensity clearly on DWI [23, 24]. This indicates that it could be more easily recognized by readers. Moreover, some studies have pointed out that T2WI in VI-RADS is mainly used for assessing tumor morphology, not for determining muscle invasion [25, 26]. Thus, DWI may provide more accurate results when T2WI and DWI scores differ.
While the value of DCE is acknowledged, especially for early prediction of chemotherapy response and identifying small lesions, its role in bladder cancer staging remains debated [12, 13, 27, 28]. Previous studies considered that DCE was important for the staging of bladder cancer [29]. However, Panebianco et al. [30] suggested that DCE may not contribute to the identification of NMIBC and MIBC. In addition, the interpretation of DCE was not friendly to less experienced readers, and additional DCE could increase the risk of their false positive rates in diagnosing MIBC. Delli et al. [12] demonstrated that less experienced readers would overestimate DCE because they were more susceptible to interference from changes around the lesion, such as inflammation, fibrosis and edema.
This study has some limitations. First, although we excluded patients whose TURBT pathology results did not reveal the detrusor muscle, the majority of patients still underwent TURBT rather than radical cystectomy. As a result, the pathological staging from TURBT may not be as accurate as that from radical cystectomy. In addition, interval follow-up is necessary for this group to confirm correct staging and assess potential upstaging over time. Second, DWI and DCE only had axial images in this study, and it was necessary to add sagittal and coronal images to further validate our conclusion. Third, we did not perform a subgroup analysis for bladder cancer. A study demonstrated that bp-MRI can be used as an alternative to mp-MRI in predicting MIBC located at the ureteral orifice [31]. However, a recent study indicated that the diagnostic performance of bp-MRI was inferior to those of mp-MRI for evaluating muscle invasion with patients with variant histology urothelial carcinoma [32]. Finally, this study was a single-center retrospective study with limited evidence, therefore multicenter and prospective studies were still required in the future.
Conclusions
mp-MRI and bp-DWI exhibit equally excellent performance in diagnosing MIBC. Furthermore, bp-DWI may demonstrate superior diagnostic performance compared to other criteria. This suggests that VI-RADS score 2 might be more appropriate than VI-RADS score 3 if T2WI scores 3 and DWI scores 2, and VI-RADS score 3 might be more appropriate than VI-RADS score 4 if T2WI scores 3 and DWI scores 3. Our findings suggest that supports the integration of bp-DWI into clinical practice as a reliable and efficient method for diagnosing MIBC. This approach not only maintains high diagnostic standards but also mitigates the limitations associated with mp-MRI. Future multicenter and prospective studies are essential to validate these findings and establish bp-MRI as a standard diagnostic tool for MIBC. The potential for bp-MRI to streamline bladder cancer diagnosis and reduce healthcare costs underscores its significant clinical value.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- NMIBC:
-
Non-Muscle-Invasive Bladder Cancer
- MIBC:
-
Muscle-Invasive Bladder Cancer
- TURBT:
-
Transurethral Resection of Bladder Tumor
- VI-RADS:
-
Vesical Imaging-Reporting and Data System
- mp-MRI:
-
Multiparametric Magnetic Resonance Imaging
- bp-MRI:
-
Biparametric Magnetic Resonance Imaging
- T2WI:
-
T2-Weighted Imaging
- DWI:
-
Diffusion-Weighted Imaging
- DCE:
-
Dynamic Contrast-Enhanced
- ADC:
-
Apparent Diffusion Coefficient (a measure used in DWI to quantify the diffusion of water molecules in tissue)
- AUC:
-
Area Under the Curve (a performance measure for diagnostic tests
- ROC:
-
Receiver Operating Characteristic (a graphical plot illustrating the diagnostic ability of a binary classifier system)
References
Sung H, et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49.
Flaig TW, et al. NCCN Guidelines(R) insights: bladder Cancer, Version 2.2022. J Natl Compr Canc Netw. 2022;20(8):866–78.
Babjuk M, et al. European Association of Urology Guidelines on non-muscle-invasive bladder Cancer (Ta, T1, and carcinoma in situ). Eur Urol. 2022;81(1):75–94.
Cumberbatch M, et al. Repeat Transurethral Resection in non-muscle-invasive bladder Cancer: a systematic review. Eur Urol. 2018;73(6):925–33.
Golan S, et al. Transurethral resection of bladder tumour complicated by perforation requiring open surgical repair - clinical characteristics and oncological outcomes. BJU Int. 2011;107(7):1065–8.
Panebianco V, et al. Multiparametric magnetic resonance imaging for bladder Cancer: development of VI-RADS (Vesical Imaging-Reporting and Data System). Eur Urol. 2018;74(3):294–306.
Yuan B, et al. Role of Vesical Imaging-Reporting and Data System in predicting muscle-invasive bladder cancer: a diagnostic meta-analysis. Int J Urol. 2022;29(3):186–95.
Asif A, et al. Comparing biparametric to multiparametric MRI in the diagnosis of clinically significant prostate cancer in biopsy-naive men (PRIME): a prospective, international, multicentre, non-inferiority within-patient, diagnostic yield trial protocol. BMJ Open. 2023;13(4):e070280.
Zhou GX, et al. Contrast-enhanced dynamic and diffusion-weighted MR imaging at 3.0 T to assess aggressiveness of bladder cancer. Eur J Radiol. 2014;83(11):2013–8.
Cho J, et al. Biparametric versus multiparametric magnetic resonance imaging of the prostate: detection of clinically significant cancer in a perfect match group. Prostate Int. 2020;8(4):146–51.
Woo S, et al. Evaluating residual tumor after neoadjuvant chemotherapy for muscle-invasive urothelial bladder cancer: diagnostic performance and outcomes using biparametric vs. multiparametric MRI. Cancer Imaging. 2023;23(1):110.
Delli PA, et al. Bladder cancer: do we need contrast injection for MRI assessment of muscle invasion? A prospective multi-reader VI-RADS approach. Eur Radiol. 2021;31(6):3874–83.
Bricio T, et al. What is the impact of dynamic contrast-enhancement sequence in the Vesical Imaging, Reporting and Data System (VI-RADS)? A subgroup analysis. Cancer Imaging. 2022;22(1):20.
Watanabe M, et al. Clinical validity of non-contrast-enhanced VI-RADS: prospective study using 3-T MRI with high-gradient magnetic field. Eur Radiol. 2022;32(11):7513–21.
Noh TI, et al. Comparison between biparametric and multiparametric MRI in predicting muscle invasion by bladder cancer based on the VI-RADS. Sci Rep. 2022;12(1):20689.
Elshetry A, et al. Diagnostic accuracy and discriminative power of biparametric versus multiparametric MRI in predicting muscle-invasive bladder cancer. Eur J Radiol. 2022;151:110282.
Feng C, et al. Evaluation of a fractional-order calculus diffusion model and bi-parametric VI-RADS for staging and grading bladder urothelial carcinoma. Eur Radiol. 2022;32(2):890–900.
Moch H, Lyon et al. France: International Agency for Research on Cancer; 2016.
Brierley JD, et al. International Union Against Cancer TNM classification of malignant tumors. Volume 8. New York, NY: Wiley-Blackwell; 2017. p. 263.
Ye L, et al. Biparametric magnetic resonance imaging assessment for detection of muscle-invasive bladder cancer: a systematic review and meta-analysis. Eur Radiol. 2022;32(9):6480–92.
Tekes A, et al. Dynamic MRI of bladder cancer: evaluation of staging accuracy. AJR Am J Roentgenol. 2005;184(1):121–7.
Wang H, et al. Multiparametric MRI for bladder Cancer: validation of VI-RADS for the detection of Detrusor muscle Invasion. Radiology. 2019;291(3):668–74.
Narumi Y, et al. Bladder wall morphology: in vitro MR imaging-histopathologic correlation. Radiology. 1993;187(1):151–5.
Wang HJ, et al. Diffusion-weighted MRI in bladder carcinoma: the differentiation between tumor recurrence and benign changes after resection. Abdom Imaging. 2014;39(1):135–41.
Aslan S, et al. Comparison of the diagnostic accuracy and validity of biparametric MRI and multiparametric MRI-based VI-RADS scoring in bladder cancer; is contrast material really necessary in detecting muscle invasion? Abdom Radiol (NY). 2022;47(2):771–80.
Panebianco V, et al. VI-RADS for bladder Cancer: current applications and future developments. J Magn Reson Imaging. 2022;55(1):23–36.
Nguyen HT, et al. Prediction of chemotherapeutic response in bladder cancer using K-means clustering of dynamic contrast-enhanced (DCE)-MRI pharmacokinetic parameters. J Magn Reson Imaging. 2015;41(5):1374–82.
Yang X, et al. Quantitative multiparametric MRI as a promising tool for the assessment of early response to neoadjuvant chemotherapy in bladder cancer. Eur J Radiol. 2022;157:110587.
Takeuchi M, et al. Urinary bladder cancer: diffusion-weighted MR imaging–accuracy for diagnosing T stage and estimating histologic grade. Radiology. 2009;251(1):112–21.
Panebianco V, et al. An evaluation of morphological and functional multi-parametric MRI sequences in classifying non-muscle and muscle invasive bladder cancer. Eur Radiol. 2017;27(9):3759–66.
Eryuruk U, Tasdemir MN, Aslan S. Comparison of the diagnostic performance of biparametric and multiparametric MRI in detecting muscle invasion of bladder cancer located at the ureteral orifice. Abdom Radiol (NY). 2023;48(10):3174–82.
Arita Y, Kwee TC, Woo S, et al. Biparametric versus multiparametric magnetic resonance imaging for assessing muscle invasion in bladder urothelial carcinoma with variant histology using the Vesical Imaging-Reporting and Data System[J]. Eur Urol Focus; 2023.
Acknowledgements
Not applicable.
Funding
This study has received funding by: National Natural Science Foundation of China. (No: 82072832、82273152); Jiangsu Province Hospital (the First Affiliated Hospital of Nanjing Medical University) Clinical Capacity Enhancement Project. (No: JSPH-MA-2022-5); Jiangsu Province Capability Improvement Project through Science, Technology and Education (No. ZDXK202219).
Author information
Authors and Affiliations
Contributions
PL, LC, LJ, and HC contributed to the conception, design, data acquisition, and drafting of the manuscript. QC, KB, RB, and QW provided statistical analysis, along with administrative, technical, and material support. Supervision of the manuscript was carried out by XY and QL. Funding acquisition was managed by QL. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Human Ethics and Consent to Participate
In accordance with the Declaration of Helsinki, the Ethics Committee of Jiangsu Provincial People’s Hospital (IRB) reviewed the study’s design and determined that ethical approval was not required due to its retrospective nature. Consequently, the committee waived the need for formal ethics approval.
Consent to Participate
Informed consent was obtained from each participant through verbal meetings or telephone follow-up.
Clinical trial number
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liu, P., Cai, L., Jiang, L. et al. Comparative diagnostic performance of VI-RADS based on biparametric and multiparametric MRI in predicting muscle invasion in bladder cancer. BMC Med Imaging 25, 60 (2025). https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12880-025-01595-3
Received:
Accepted:
Published:
DOI: https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12880-025-01595-3